Medication-Assisted Treatment in Pregnancy
April 20, 2020
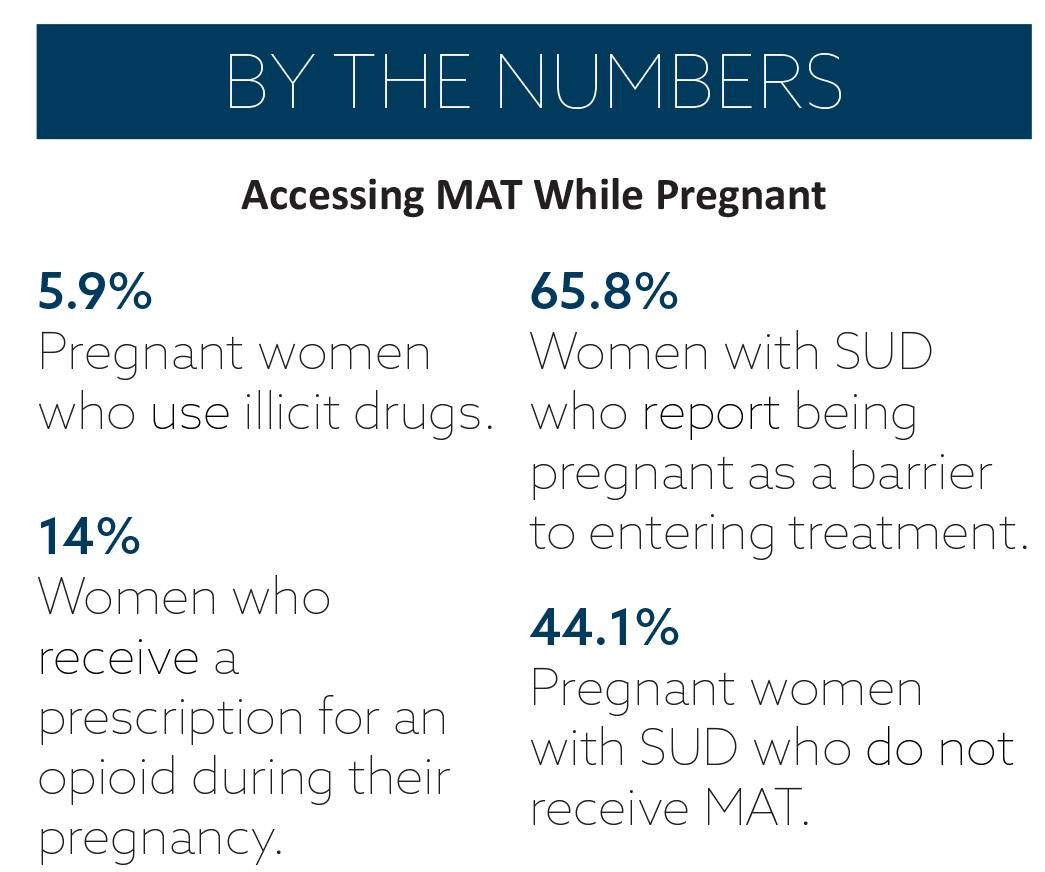
Medication-assisted treatment (MAT) is an evidence-based treatment protocol for people with substance use disorder (SUD). MAT prevents the onset of withdrawal, which can be harmful to both pregnant women and their babies. Pregnant women with SUD face elevated risks of poverty, psychiatric disorders, and intimate partner violence and, once they give birth, issues like a lack of specialized postpartum treatment options and ongoing discrimination. MAT has been shown to improve patient survival, increase retention in treatment, decrease illicit opiate use and other criminal activity, increase patients’ ability to gain and maintain employment, and improve birth outcomes among pregnant women with SUD.
For pregnant women with SUD, access to MAT is complicated by several factors, including where they live in relation to healthcare facilities, whether or not they are covered by private or public insurance, and their jurisdictions’ child abuse and neglect laws. Additionally, the criminal justice, healthcare, and social services systems often struggle to appropriately respond to the needs of pregnant and postpartum women struggling with SUD. Fear of being arrested, losing custody of their child(ren), and other consequences further prevent pregnant and postpartum women with SUD from accessing MAT.

Legislative Trends
Recent state policy trends regarding access to MAT for pregnant women with SUD focus on implementing treatment programs, allocating funds for treatment services, and enhancing consumer and provider awareness. These policies reflect the understanding that a coordinated and collaborative approach is necessary to meet the complex needs of pregnant and parenting women with SUD.
Program Implementation
In 2019, Oregon enacted legislation authorizing the health authority to establish a pilot program for offering treatment, including MAT, to pregnant women. The legislation notes that the pilot program can include the use of peer mentors and doulas, as well as any necessary SUD treatment, during the first year of an infant’s life.
In Texas, a bill passed directing the health department to (1) increase access to MAT for women with opioid use disorder (OUD) during pregnancy and the postpartum period, and (2) prevent OUD by reducing the number of opioid drugs prescribed before, during, and following a delivery. In Maryland, the governor signed a bill requiring each local correctional facility to assess the mental health and substance use status of each inmate to determine if it’s appropriate to diagnosis OUD and, if so, whether MAT is appropriate. Per the bill, each pregnant woman identified with OUD will receive evaluation and be offered MAT as soon as it is feasible.
Funding and Coverage
 Colorado’s legislature found that facilities providing treatment (including MAT) to individuals with SUD and clinics providing obstetric and gynecologic care would better serve pregnant and postpartum women if their services were provided at the same location. As a result, the legislature passed a bill creating a maternal and child health pilot program, which provides grants to treatment facilities and clinics to integrate behavioral health, including SUD treatment and MAT, and obstetric and gynecologic care. In Indiana, a bill was introduced that would appropriate $1 million to continue an opioid addiction recovery pilot program. If passed, the permanent program would be expanded to include addiction treatment (including MAT) for pregnant women and women with a newborn seeking assistance for recovery from OUD. Lastly, Maine enacted legislation preventing carriers from imposing prior authorization requirements on pregnant women for MAT for OUD.
Colorado’s legislature found that facilities providing treatment (including MAT) to individuals with SUD and clinics providing obstetric and gynecologic care would better serve pregnant and postpartum women if their services were provided at the same location. As a result, the legislature passed a bill creating a maternal and child health pilot program, which provides grants to treatment facilities and clinics to integrate behavioral health, including SUD treatment and MAT, and obstetric and gynecologic care. In Indiana, a bill was introduced that would appropriate $1 million to continue an opioid addiction recovery pilot program. If passed, the permanent program would be expanded to include addiction treatment (including MAT) for pregnant women and women with a newborn seeking assistance for recovery from OUD. Lastly, Maine enacted legislation preventing carriers from imposing prior authorization requirements on pregnant women for MAT for OUD.
Education and Awareness
In 2018, New York passed legislation establishing the Children and Recovering Mothers program, which supplies healthcare providers and expectant mothers with information on treating OUD during pregnancy. The program is modeled after the Children and Recovering Mothers (CHARM) Collaborative originally developed in Vermont. The CHARM model is an interdisciplinary and cross-agency team effort to coordinate care for pregnant and parenting women with a history of OUD.
In May 2019, Washington state’s governor signed a bill requiring all approved opioid treatment programs to provide services to pregnant women and to disseminate information regarding how opioid use and OUD medication may contribute to neonatal opioid dependence and subsequent withdrawal.
Looking Ahead
 ASTHO expects states to continue exploring legislative approaches to increasing access to MAT for pregnant and postpartum women with SUD. Future state policy action may include:
ASTHO expects states to continue exploring legislative approaches to increasing access to MAT for pregnant and postpartum women with SUD. Future state policy action may include:
- Building public health workforce capacity by training and placing peer recovery coaches, developing increased MAT waiver training for physicians, and implementing policies that encourage all providers (regardless of specialization) to refer a patient to treatment (known as “no wrong door” policies).
- Eliminating provider-stigma against pregnant and postpartum women with SUD through education, training, and MAT credentialing requirements.
- Establishing and implementing innovative service delivery strategies (such as integrating or co- locating MAT within other healthcare services), developing guidelines and best practices for MAT among pregnant women, and appropriating sufficient funding for MAT services.
- Helping to connect pregnant and postpartum women with SUD treatment and decriminalizing potential pathways into treatment through innovative programming (such as Kentucky’s PATHways program, syringe service programs, drug courts, or expanded MAT prescribing) or policies (such as Casey’s Law in Kentucky or the Angel Program in Massachusetts).
Through such comprehensive and innovative policies, states are well-positioned to improve MAT access for pregnant and parenting women and continue the strategic and effective abatement of the opioid epidemic.